Qualis Health Award Project presented by Hal J. Mason RT, R, CT, CT Technologist at Yakima Memorial Hospital, Valley Imaging Outpatient Imaging Center in Yakima, Washington.
Description of organization: Valley Imaging is Yakima Valley Memorial Hospital’s outpatient imaging center located in Yakima, Washington. Our 225 bed not-for-profit campus hospital serves more than 130,000 patients annually. We provide comprehensive medical and surgical care, teamed with advanced technology to provide patients with modern and immediate attention to acute medical needs.
PROJECT TITLE: Computerized Tomography Radiation Dose Reduction Project.
SUMMARY: The use of CT scanning has been steadily increasing over the last 15+ years. Nationally CT scans are responsible for over 40 percent of the cumulative diagnostic radiation exposure to patients. YVMH developed a CT dose reduction project that was and remains committed to improving patient safety through the application of ALARA (As Low As Reasonably Achievable) in every CT dosing decision. To date, measuring from the beginning of the project, we have reduced harm to the patient by reducing the radiation exposure by 40 to 60 percent over the spectrum of CT exams performed at YVMH. We reduced dose by using a combination of initial and on-going dose management education, DLP reduction by raising image noise factors and the use of leveraging technology (MEDICVISION SafeCT) to improve image quality
WHY NEEDED: Following numerous articles and presentations in national news media about excessive radiation exposure in CT exams we decided to undertake an examination of our CT dose exposure levels. While not terribly excessive we felt that we could reduce the CT radiation dose to the patient. Our then current dose levels were in keeping with the Washington State Department of Health guidelines for maximum CTDI(CT dose index) Volume values recommended by the American College of Radiology. The maximum recommended values of CTDI were overly generous for our scanners so we felt it would be appropriate to undertake a CT dose reduction project that would yield lower exposure levels and still have high quality CT images available for the Radiologist interpretation. To understand where we were in regard to CTDI and DLP(dose length product) dose levels we retrieved about two years of recorded dose reports from the full spectrum of CT scans performed at our facilities. This record of thousands of scans formed a robust baseline of exposure levels that we could use as a starting point for dose levels needed to get high quality images based on the dose records in comparison to Radiologist CT scan interpretations.
DESCRIBE MEASURE AND METHODS USED FOR COLLECTING DATA AND INFORMATION: By keeping specific DLP and exposure technique records and comparing those figures to image quality we began to see that we could raise the noise index and lower the MA hence reducing dose to the patient. A major concern during the initial phase of this dose reduction project was how to maintain satisfaction with image quality by the interpreting Radiologist. After discussion with our chief CT Radiologist, Dr. Feldmann, we decided to trickle in the exposure level decreases very slowly to allow the interpreting Radiologist to become accustomed to the higher noise levels of the images. By keeping the process of raising noise levels very slow, nearly one year, we encountered virtually no resistance by the Radiologists to the gradual change in image appearance. The slow introduction of change was a very important part of the dose reduction strategy. We did want to start a resistance campaign on the part of the interpreting Radiologists. We finally reached a limit on what we could achieve by the increase in noise levels and MA reduction. CT scans that were compromised by out of field artifact or patient size were the first to show a marked decrease in image quality. When noticeable changes in normal CT scans became obvious we held the noise and technique level changes at a point where we achieved an average of 28.6 percent exposure reduction. We held this level for several months as we gradually continued to refine our CT protocols to yield the lowest possible CTDI and DLP. The noise index changes we made were held to a maximum of 3 percent for any one change. The changes we made were left in place for at least two weeks to allow the Radiologists to adjust to the increase in image noise. We did not selectively apply the changes but changed the entire spectrum of CT protocols each time. Since the perception of image noise is by nature very subjective our Radiologists opinions of the image quality we were achieving was at all times of primary concern. To be sure that the quality of our scans was maintained we kept a record of our CT scanner QA performance both at the original technique level and at the level of noise increase at each 3 percent change. At no point did we find that the change in noise level changed the Hounsfield numbers of the phantom used for QA testing. Our biggest challenge during the development of the project was making changes to the CT protocols slow enough so that the interpreting Radiologists remained unaware the change was happening. The records kept during the initial effort were scan dose reports, CTDI volume and DLP for each scan. In addition we kept DLP/mm of tissue averages for three scanners. The DLP/mm of tissue was used to even out patient differences in BMI, age and physique. The dose reductions we achieved during this phase of the project directly related to the increase in image noise. In other words, noise up= energy down, now at what point do you have to stop these changes so you do not loose acceptable image quality.
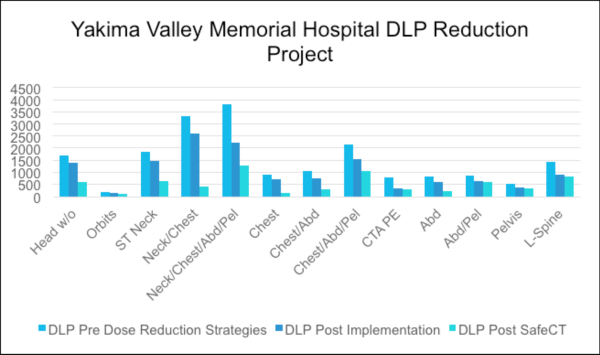
Click the chart for more information.
SUMMARY OF SYSTEM OR PROCESS CHANGES MADE BASE ON DATA OR INFORMATION COLLECTED:
Initial noise/ MA changes. What we learned from the initial noise and MA changes was that it took at least a 15 percent increase in noise and subsequent decrease in MA before we noticed any change at all in the image quality. This led us to think that at the initial exposure settings across the full CT spectrum we were using too much MA to get acceptable images. Images are not made increasingly good by using excessive MA settings. You reach a point of no image quality increase where more technique does not improve normal scans, all you do is over expose the patient to ionizing radiation. The question became at what point in energy reduction do you begin to see an image quality reduction and how much of an image noise increase and MA reduction can the interpreting Radiologist tolerate. Our initial technique changes of 3 percent at a time were tolerated until we reached a 20 percent change. At that point we reduced the rate of change to just over one percent at a time and held the change for at least two weeks before another change was made. This method worked well until we got to about a twenty five percent reduction in exposure. At that point we began to get complaints of excessive noise in the images from the interpreting Radiologists. At this point in order to reduce ionizing radiation exposure further we had to start using some type of iterative reconstruction product to improve the quality of the CT images. At RSNA (RADIOLOGY SOCIETY OF NORTH AMERICA) our Radiologists discovered the MEDICVISION SafeCT product that could be used to improve the image quality of high noise low MA CT images. YVMH decided to acquire the MEDICVISION SafeCT product in 2012. After we had the SafeCT product in place we carefully evaluated the resulting CT images for quality improvement. It took some time for the Radiologists to adjust to the appearance of the SafeCT images. After about three months we again began to raise the noise index to lower the MA and CTDIvol/DLP. We made these changes at one to two percent at a time again leaving the change in place for at least two weeks. We were able to gain a further increase in noise of about twenty five percent after the implementation of the SafeCT product until we noticed a decrease in image quality. At this point we backed off the noise increase about five percent so the noticeable image quality decrease disappeared. Throughout the course of the SafeCT product introduction extensive records of image exposure factors were recorded. We recorded DLP per exam, DLP per mm of tissue for exam catagories , CTDIvol per exam, m/Sv per exam. We also followed up with the Radiologist interpretation report for any comment regarding poor exam quality. In addition to the recording and evaluation of dose data many image review sessions were held with the lead CT Radiologist to evaluate image quality. At this time, late fall of 2013 we are holding any further changes to the CT scan exposure factors. Using the CT platforms we currently have in place we think that we have maximized the performance of all of our available technology to yield the lowest possible ionizing radiation exposure levels to get the highest quality of CT images for our patient population.
HOW DOES THIS PROJECT PROVIDE BETTER CARE FOR PATIENTS: Every patient that comes to YVMH for physician referred CT imaging receives the lowest ionizing radiation dose, highest image quality CT scans available from our CT equipment. Our radiation dose exposure levels are supported by lengthy and robust data accumulation and evaluation.
Pursuing the dose reductions in CT imaging is in keeping with a primary responsibility that Radiologic Technologists have to the entire patient population. That is ALARA, all ionizing radiation exposures should be kept “As Low As Reasonably Achievable”. The national radiology campaigns of IMAGE GENTLY for pediatric patients and IMAGE WISELY for all other patients support and endorse efforts to limit radiation exposure to all patients. By utilizing available technology and making the effort to provide on- going dose reduction education to our CT staff we continue to meet our obligation to our patient population of providing the very best CT imaging.
REDUCING COSTS: During the initial dose reduction phase of the project and prior to the introduction of SafeCT we found that substantial gains in radiation exposure reduction can occur by optimizing exposure factors and evaluating image quality. These steps are available to any CT users at virtually no cost. Changes made as described provide direct benefit to the patient population. In order to get the most dose reduction possible to limit exposure we had to acquire an iterative image reconstruction product to improve image quality. Any acquisition of a product that does not generate immediate income is a commitment by the responsible institution that what is best for the patient is ultimately what is best for everyone.
DESCRIPTION OF INNOVATION: Taking the time to do a substantial dose reduction project and procure leveraging technology to improve image quality is a statement of desired excellence by a health care institution. Our innovation is that for the CT platforms we are using we are achieving exceptionally low ionizing radiation exposure levels. This requires a commitment by CT Technologists, hospital management and by Radiologists to make the effort to provide the lowest possible radiation exposure to all patients. By examining exposure records, dose reports and image quality from other CT services and in comparison to ours we have achieved our goal of “the very best images for the very least exposure”.
Some blogs you may have missed:
- Concern Over Radiation Risks from CT Imaging?
- Mobile CT brings low-dose lung cancer screening to underserved
- Role of iterative reconstruction technique for low dose chest CT
- Are you prepared for mandatory CT dose tracking?
- Failure to meet new dose reduction standards could jeopardize #Medicare dollars



